UPMC Digital Pathology CME Courses
CME Credit Hours: 0.50
Target Audience:
Pathologists, Pathology Residents, Medical Students, Pathology Assistants and Pathology Assistant Students
Educational Objectives:
Upon completion of this activity, participants will be able to:
- As a result of participation in this activity, participants will be able to increase awareness of the pathologic evaluation of multinucleated cells along with a smaller tumor cell population.
Additional Readings:
- Ichikawa T, Wakisaka A, Daido S, et al. A case of solitary subependymal giant cell astrocytoma: two somatic hits of TSC2 in the tumor, without evidence of somatic mosaicism. J Mol Diagn. 2005; 7(4):544-549.
- Takei H, Adesina AM, Powell SZ. Solitary subependymal giant cell astrocytoma incidentally found at autopsy in an elderly woman without tuberous sclerosis complex. Neuropathology. 2009; 29(2):181-186.
- Grajkowska W, Kotulska K, Jurkiewicz E, et al. Subependymal giant cell astrocytomas with atypical histological features mimicking malignant gliomas. Folia Neuropathol. 2011; 49(1):39-46.
- Svajdler M, Jr., Deak L, Rychly B, Talarcik P, Frohlichova L. Subependymal giant cell astrocytoma with atypical clinical and pathological features: a diagnostic pitfall. Cesk Patol. 2013; 49(2):76-79.
- Al-Saleem T, Wessner LL, Scheithauer BW, et al. Malignant tumors of the kidney, brain, and soft tissues in children and young adults with the tuberous sclerosis complex. Cancer. 1998; 83(10):2208-2216.
- Vignoli A, Lesma E, Alfano RM, et al. Glioblastoma multiforme in a child with tuberous sclerosis complex. Am J Med Genet A. 2015; 167A(10):2388-2393.
Authors:
Daniel Marker, MD, PhD
Release Date: 2022-06-14
Review Date: 2024-06-14
Expiration Date: 2025-06-14
No relationships with industry relevant to the content of this educational activity have been disclosed.
The University of Pittsburgh School of Medicine is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians.
The University of Pittsburgh School of Medicine designates this enduring material for a maximum of 0.50 AMA PRA Category 1 CreditsTM. Each physician
should only claim credit commensurate with the extent of their participation in the activity.
Other health care professionals are awarded ( 0.05 ) continuing education units (CEU) which are equivalent to 0.50 contact hours.
Presenters for this program have been requested to identify financial or other relationships with manufacturer(s) of any commercial product(s) or with provider(s)
of any commercial service(s) which, in the context of their topics, could be perceived as real or apparent conflicts of interest.
The University of Pittsburgh is an affirmative action, equal opportunity institution.
Case 1072 - A Young Patient with a History of Intermittent Headaches and Fevers
Contributed by: Daniel Marker, MD, PhD
A maximum of 0.50 AMA PRA Category 1 Credits are available from a quiz on this case from the University of Pittsburgh's Internet-based Studies in Education and Research.
This course is eligible for the American Board of Pathology SAM credit
Click here to take the quiz and
earn 0.50 AMA PRA Category 1 Credits
Please review the case before taking the quiz. The site will now ask for your ABPath MOC number before taking the quiz if it was not supplied previously.
CLINICAL HISTORY
A young previously healthy child with no significant medical history presented to their primary care physician with a history of intermittent headaches and fevers for the past few months. The headaches had no predictable pattern and no positional triggers or intensity change. The patient was initially treated with oral antibiotics, which failed to improve their symptoms. They then developed gait disturbances and visual changes, prompting imaging studies (Figures 1 and 2).
MRI of the head revealed a 5.8 x 4.2 x 4.1 cm heterogenously enhancing lobulated mass in the right lateral ventricle that involved the right frontal lobe periventricular white matter and abutted the right thalamus. There was extensive surrounding vasogenic edema and partial obstruction of the foramen of Monroe resulting in mild lateral ventriculomegaly. The patient was referred to Children's Hospital of Pittsburgh and taken to the OR for tumor resection.
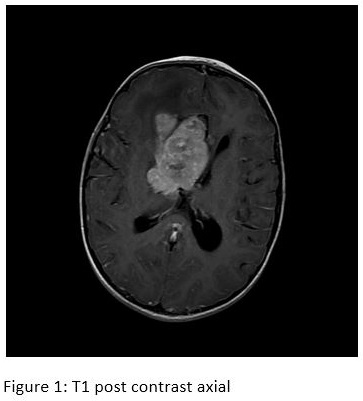 Figure 1 |
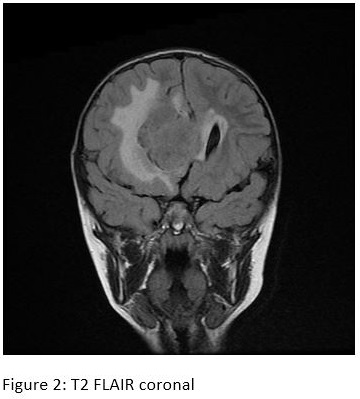 Figure 2 |
MICROSCOPIC DESCRIPTION
Intraoperative smear
The intraoperative smear showed huge bizarre multinucleated cells along with a smaller tumor cell population. Mitotic figures were present and the dirty background was concerning for necrosis. The differential diagnosis included high-grade primary brain tumor versus metastatic poorly differentiated tumor from unknown primary. The intraoperative diagnosis was, "morphologically bizarre tumor, defer to permanents."
Permanent H&E
Permanent sections showed the same huge bizarre tumor cell population with small cell component. Extensive necrosis was present. No definitive parenchymal infiltration was identified. The tumor cells showed patchy positivity for GFAP and were negative for Olig2, TTF1, synaptophysin, Cam5.2, EMA, Sox-10, and Gata3, although the interpretation of the immunostains was limited by extensive cautery artifact. TP53 was suspicious for clonal loss. The Ki67 proliferation index was approximately 30%. Molecular analysis of the tumor was performed and identified stop-gain mutations in TP53, RB1, and TSC2.
Please click the "Final Diagnosis" tab at the top of the screen to view the rest of the case.
FINAL DIAGNOSIS
High-grade Subependymal Giant Cell Astrocytoma (SEGA).
DISCUSSION
SEGAs are classically WHO grade 1 intraventricular lesions that occur in patients with tuberous sclerosis complex (TSC, germline mutations in either TSC1 or TSC2). Rare sporadic cases have been reported.1,2 The patient in this case had no other stigmata of TSC and has not undergone germline testing. SEGAs are histologically characterized by large gemistocytic-like cells with admixed small tumor cells and lymphocytes with a sharp brain to tumor interface. Proliferative indices are often low. These tumors tend to occur in young patients and can be the presenting symptom of TSC. Presenting clinical symptoms included obstructive hydrocephalus, hemorrhage into the lesion, or seizure. Gross total resection is generally curative and recurrences are rare.
High grade SEGA or anaplastic transformation of a low-grade SEGA is exceedingly rare, with only a few case reports describing these entities.3,4 This case shows marked pleomorphism and anaplasia, far beyond what is normally seen in SEGA, as well as high proliferation and necrosis. The main differential diagnostic consideration in this case was glioblastoma, which can also occur in patients with TSC.5,6 The determining diagnostic factor in favor of high-grade SEGA was the lack of definitive brain invasion, and the presence of a sharp brain to tumor interface on a subsequent resection specimen received around the time of the molecular results. The prognosis for this very rare lesion is not clear.
Click here to take the quiz and
earn 0.50 AMA PRA Category 1 Credits
Please review the case before taking the quiz. The site will now ask for your ABPath MOC number before taking the quiz if it was not supplied previously.